Programs Application Form
About Us
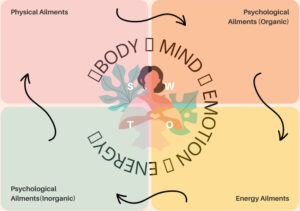
In today’s world, the idea of health and medicine is of instant relief. It is the impatience and fear of the unknown that drives this feeling of wanting everything in ‘Fast Track’. When we talk about health, it is holistic, all these things mentioned have to be aligned within this Organism: Body, Mind, Emotion & Energy. Ill health, therefore, is a misalignment of these faculties with each other. And it takes time and effort to align these key aspects for the proper functioning of a being. There are some natural laws which healthcare has to consider before diagnosing and treating an individual. This consideration and holistic approach will lead to disease relief, prevention and sustenance of recovery. Today, Quantum science is saying this human system is a holographic expression continuum of THOUGHT, EMOTION and ACTION. Therefore Medical Sciences have to be integrated in terms of methods and bylaws. Therefore, The future of healthcare is Quantum and holistic healthcare. Our doctors prescribe only what is very much needed and provide distinct healthy methods physically, mentally and energy-wise. Most diseases are internal and chronic. read more….
Centre of excellence
Contact Info
AMRF COMPLEX, Gatih Yoga Centre | Malikuchi | PO- Digheli | Near Girin Choudhary – 781334 | Nalbari Assam | CINU85110AS2019PTC019756
+91 7002197551
AMRQHTM Lifeline
+91 9395760851
AMRQHTM Emergency
+91 7002197551
AMRQHTM Emergency
+91 8822341009
AMRQHTM Reception/Quick appointment
+91 7896769522
AMRQHTM Patient-influx surveillance
+91 9395653856
AMRQHTM International Patient control
amrfhospital@gmail.com
Site-map